

by James Lyons-Weiler, PhD, Popular Rationalism, ©2025

(Jun. 6, 2025) — Here are the facts as can best be found in the scientific record. The exonerating studies on pertussis vaccines and SIDS have problems.
DTP Raised Deadly Vaccine Concerns in 1970s Japan
In the early 1970s, Japan’s routine immunization schedule included the combined diphtheria, tetanus, and pertussis (DTP) vaccine beginning in infancy (around 3 months of age). During this period, reports of serious adverse reactions to the whole-cell pertussis component of DTP began to alarm the public. In 1974 and 1975, two infants in Japan died within a day of receiving DTP, triggering public fear and increasing vaccine risk awareness. By 1975, health authorities reacted by suspending infant pertussis vaccinations and raising the minimum DTP vaccination age from 3 months to 2 years. This effectively halted routine pertussis immunization for babies and was a dramatic policy shift aimed at improving vaccine safety.
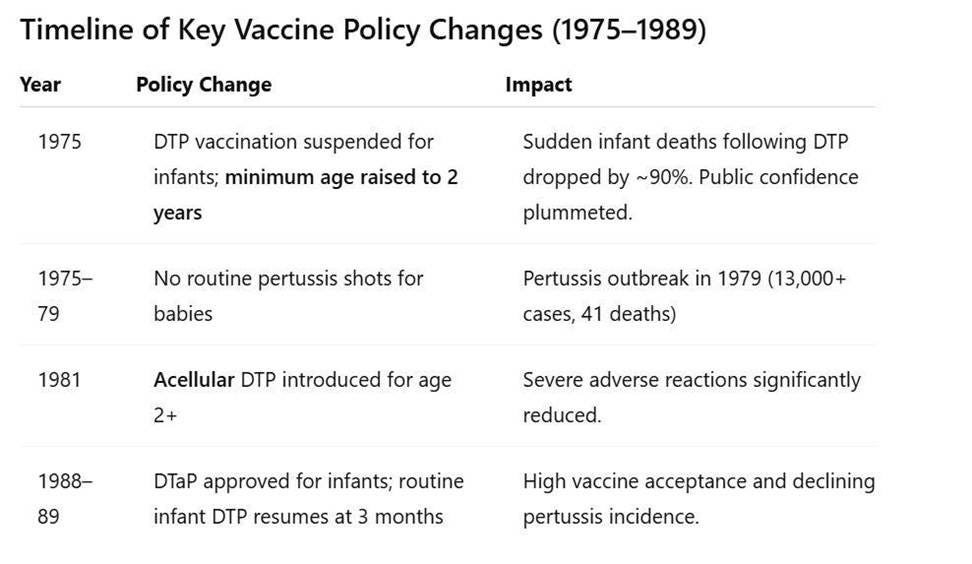
Timeline of Key Vaccine Policy Changes (1975–1989)
In 1975, DTP vaccination was suspended for infants. After infant deaths were linked temporally to DTP, the government temporarily halted pertussis immunizations. The program was revamped to delay DTP until age 2 (instead of infancy). As a direct result, reports of sudden deaths following vaccination virtually disappeared in the ensuing years. In fact, vaccine injury compensation for post-DTP sudden deaths dropped from 37 cases (1970–1974) to only 3 cases in the period 1975–1981. According to an American Academy of Pediatrics task force, the category of “sudden death” as a vaccine-related report “disappeared…when immunization was delayed until a child was 24 months of age” (Cherry et al., 1988). This delay also markedly reduced other severe adverse reactions temporally associated with DTP in infants.
(It is worth noting that Cherry et al. (1988) is a secondary analysis conducted by a U.S.-based AAP task force and not based on original Japanese health system records. Its interpretation reflects Western diagnostic conventions and may not fully represent Japanese reporting practices of the time.)
By the late 1970s, Japan saw a pertussis resurgence. The curtailment of infant DTP led to a steep decline in pertussis vaccination coverage. Consequently, whooping cough (pertussis) cases surged. In the three years before the 1975 suspension, Japan had only about 400 pertussis cases and 10 deaths; in the three years after stopping infant shots, cases spiked to over 13,000 with 113 deaths. A major nationwide pertussis outbreak in 1979 infected tens of thousands; 41 infant deaths were attributed to pertussis. This tragedy underscored the vaccine’s benefits – a point recognized by the public and government in hindsight.
In 1981, the acellular pertussis vaccine (DTaP) was introduced. In response to safety concerns, Japan became the first country to develop and approve an acellular pertussis (aP) vaccine – a safer formulation containing purified pertussis components instead of whole bacterial cells. Starting late 1981, acellular DTP (often called DTaP) completely replaced the old whole-cell DTP for routine use. Initially, the acellular vaccine was given only to children age 2 years, continuing the policy of delayed start. From 1982–1988, over 40 million doses of acellular pertussis vaccine were administered to Japanese 2-year-olds (Watanabe & Nagai, 2005). Studies confirmed that serious adverse events, including encephalopathy, convulsions, and sudden deaths, were significantly lower with the new acellular DTP compared to the reactogenic whole-cell vaccine (Kuno‐Sakai & Kimura, 2004).
However, acellular pertussis vaccines are also known to reduce symptomatic disease without preventing colonization or transmission. As such, post-vaccine case counts likely underestimated the true burden of circulating Bordetella pertussis, especially among asymptomatic carriers. It is worth noting that because aP vaccination is known to mask infection, and ‘cases’ in the vaccinated exclude asymptomatic infected (Warfel et al., 2013). This is especially problematic because only symptomatic individuals – including healthcare workers- will seek treatment (antibiotics) and self-quarantine to avoid making infants, the most vulnerable population, sick.
In the late 1980s (1988–1989), Japan resumed infant immunization. As confidence in the acellular DTP grew, Japanese health authorities began to move the pertussis vaccine back into infancy. In 1988 the Ministry of Health approved DTaP for infants, and by 1989 many areas of Japan re-introduced the pertussis shot at 3 months of age as part of the routine schedule. Thus, after roughly 14 years of delayed vaccination policy, Japan returned to vaccinating infants in early life – but now with DTaP. High vaccine acceptance was achieved, and pertussis incidence sharply declined again by the 1990s. (For reference, in 1994 Japan formally amended its Immunization Law to end mandatory vaccination, but it continued strong recommendations for all infant vaccines, including DTaP, under age 2.)
SIDS Rates Before, During, and After the Changes
Sudden Infant Death Syndrome (SIDS) – the unexplained sudden death of an apparently healthy infant – was relatively uncommon in Japan during the 1970s and 1980s, especially compared to Western nations. It is important to note that diagnostic practices differed: Japanese authorities often classified unexplained infant deaths under categories like “unknown cause” or suffocation, meaning not all such deaths were formally labeled as SIDS (Sawaguchi et al., 2000). Nonetheless, available data suggest some notable trends around the time of the vaccination policy changes:
Early 1970s (pre-change): With DTP given at 3 months, there were documented cases of infants dying suddenly soon after vaccination. In 1970–1974, Japan recorded 37 infant “sudden deaths” temporally associated with pertussis shots (about 1.47 deaths per million DTP doses). These cases likely would be classified as SIDS or vaccine-related SIDS by today’s standards. They represented a small fraction of overall infant deaths, but their clustering shortly post-vaccination raised national concern.
Late 1970s to mid-1980s (during delay period): After 1975, with no infants being immunized against pertussis in their first two years, reports of sudden deaths following vaccination virtually vanished. Japan’s vaccine injury data show that post-immunization sudden death cases fell by ~90% once the DTP series was deferred to age 2 . Indeed, James Cherry’s review noted that “‘sudden death’…disappeared” as a reported phenomenon when infant DTP was removed. In epidemiologic terms, Japan’s SIDS rate during the late 1970s and 1980s remained very low, on the order of only a few tenths of a death per thousand births (Müller-Nordhorn et al., 2020). One international analysis found that unlike many Western countries that saw a mid-1980s peak in SIDS, Japan’s recorded SIDS mortality stayed low throughout the 1980s. For example, by the mid-1980s (1984), Japan’s SIDS rate was roughly 0.4 per 1,000 live births – well below rates in the U.S. or Europe at that time. This low incidence coincided with the period when babies were not receiving DTP in early infancy. Some have interpreted this as a mere correlation: i.e. that delayed vaccination appeared to contribute to lower SIDS occurrence.
Japan began vaccinating infants again by 1989, and through the early 1990s the recorded SIDS rate did increase somewhat. SIDS reached an observed high around the mid-1990s (approximately 0.44 per 1,000 in 1995). Notably, this time period was a peak for SIDS in many countries and also when Japan first aligned with Western-style infant sleep practices. After 1995, however, Japan’s SIDS incidence declined sharply, dropping to about 0.24 per 1,000 by 2001. By the 2000s, SIDS (as an official category) was exceedingly rare in Japan (roughly 0.1 per 1,000, or 0.01%). The halving of SIDS rates from the mid-1980s to early 2000s was largely credited to public health interventions – especially a nationwide “Back-to-Sleep” campaign in the late 1990s that encouraged non-prone sleeping and raised awareness of SIDS risk factors. In short, Japan’s continued long-term decline in infant sudden deaths after the 1980s is attributed more to safe sleep practices and other risk reductions than to vaccination policy.
It is difficult to say with certainty how much the 1975–1988 vaccine delay policy affected Japan’s overall SIDS statistics. The temporal association is more than intriguing: during the years when virtually no infants received DTP, SIDS diagnoses were extremely infrequent. However, absolute SIDS numbers in Japan were already low, and other factors (like diagnostic criteria and broader infant care improvements) likely played a major role. By the mid-1980s, Japan’s overall infant mortality rate had fallen dramatically, from about 12–13 per 1,000 in 1970 to ~5 per 1,000 in 1985 (World Bank, 2023). This 60% improvement was driven by advances in neonatal care, infection control, and living standards, which also would have reduced many causes of infant death (including SIDS). In essence, SIDS was a very small contributor to infant mortality in Japan throughout the 1970s–80s, making it challenging to isolate the effect of any single factor like vaccines on its incidence.
Read the rest here.